


I’ve known entirely too many alcoholics that have had too many wake-up and come-to-Jesus moments, only to go back to drinking as soon as the immediate crisis is over. Change only comes when the alcoholic wants to change for their own reasons, not due to external factors.
Livers are a limited resource. Wasting a donor’s liver on a person that
usis unlikely to stop drinking–despite their protestations–means that another person doesn’t get one. It may seem like a cruel calculus, but it’s the only reasonable way to ration a scarce resource. It doesn’t matter if alcoholism is a disease, or you think that it’s a moral failing; the end result is the same.deleted by creator
Healthcare is for profit. Doctors, nurses, surgeons, consumables, hospitalization, antibiotics, follow ups all get charged to OHIP at a profit for the healthcare provider.
If we had actual public healthcare, where hospitals and doctors are not private businesses, maybe we could spend more mony on treatment and rehabilitation for problem cases.
As an alcoholic, I initially agreed. Don’t waste a liver on me. Then this:
Even pleas for a living liver transplant, with Allan offering to be her donor, were not entertained.
What the actual fuck.
A partial liver transplant wasn’t viable for someone this sick, so when the partial transplant failed, they would have to resort to a full transplant from a dead donor, or she would die in operation.
Since she wasn’t eligible, a partial transplant was just a death sentence.
Liver failure is terminal. She was invariably going to die without the transplant. She wanted to receive the donation, her donor wanted to donate. If the success rate for a living transplant is zero that’s one thing, but that’s not being claimed here since she wasn’t eligible for procedural reasons.
They said it was viable in the early stages, and with a decent success rate. Just not the success rate they wanted, and for some daft reasons you need to be eligible for a full transplant from a dead patient to get a partial transplant from a living donor. Makes no sense.
I’d have supported her paying out of pocket to use the live donor that was willing, but not to use my tax money when it’s pretty fucking clear she has no intention of changing.
It’s the same reason I’m largely against the Liberal’s diabetes funding - ~90% of diabetics are Type 2 (I’m willing to help Type 1’s out because it’s not their fault) and the vast, vast majority of those are from unhealthy lifestyle even if they are genetically predisposed.
If were going to have a public health system, people should be required to take care of themselves. And no, I’m not talking about the one-off accidents from riskier activities (although I do think people should bear the cost of their own healthcare if it’s the result of criminal activities), I’m taking the problems that occur as a result of abusing your body for years or decades.
You’ve gotten a lot of downvotes but rather than doing that I want to explain to you why your position here is flawed.
First think of every lifestyle activity whether it be food, motorcycle riding, music, etc. Now consider that there are some activities that are statistically safer than others.
If we took your position to the point of being law why would we stop at food lifestyle choices? Why not just any risky lifestyle choices? Eventually you end up with a society where individuals have less choice and freedom and are constantly obligated to live the safest possible lives.
You and I both know that isn’t a desirable outcome. We should be empowering people to live the lives they choose and encouraging them to be healthy, not punishing them for make the “wrong” choice.
I attempted to address this but perhaps I wasn’t clear:
Yes, some activities are risky then others, however many of them have absolutely 0 negative impact on you unless something major happens all at once. In fact, many of them have major health benefits for the vast, vast majority of participants.
Contrast the above to overeating, chronically eating stuff that’s not good for you (ex. excessive sugar, salt), drinking too much, doing lots of drugs, smoking… that kind of behaviour will basically screw up everyone who partakes given enough time and has no positive health benefits at all.
You talk about a loss of freedom… I’ve already lost freedom by paying for a bunch of people who purposely fuck themselves up for no tangible benefit to themselves. There is stuff that would be good for me that I literally can’t afford because of the amount of taxes I pay.
Here’s an idea for your route of encouraging healthy lifestyle rather than removing freedom: include a physician form in my taxes where my doctor attests that I am generally in good shape (given my age) and he has no reason to believe I am doing anything that is a risk factor for chronic cardiovascular or lung diseases, diabetes or related chronic illnesses, and give me a significant tax break for doing so.
Consider what you just said can apply to motorcycling or buying a classic car with outdated safety features. There is no tangible health benefit to motorcycling or driving a classic car, it basically “has no positive health benefits at all” (as per your own words) and only increases risk. Show it be banned? What about every other risky hobby? If not, then neither should eating junk food which is measurably less dangerous/risky. Keep in mind that for smoking the overall trends of diminishing smoking habits in younger generations basically highlights the proof that encouraging healthy habits rather than punishing the individual is the correct way to approach this.
Buying a motorcycle or classic car doesn’t necessarily lead to injury in the same way that overeating and being lazy to the point of becoming a land whale does.
Being a judgmental asshole increases your likelihood of being assaulted. I shouldn’t have to pay your medical bills when you get punched in the face by a stranger.
Free expression bud, it’s my right to be a judgemental asshole. Take that up with Pierre Trudeau.
I suggest you look up just how often motorcycle injuries/deaths happen. What you’re saying only applies if you never get into an accident or fall off the bike ever, in the entire period it is owned (which could be 20-30 years). Something which is incredibly unlikely. From the language you’re using (i.e whale) I’m getting the impression that your position isn’t rational and instead based on a dislike of overweight people. I’ve done what I can here but I don’t think you’re messaging back in good faith and don’t want to entertain the perspective of someone who tries to put others beneath them based on their body and eating habits.
I’d be willing to bet that the number proportion of motorcycle owners with health problems caused by riding is a hell of a lot lower than the proportion of people who don’t eat right and don’t exercise enough and have health problems linked to that.
And no, it’s not just overweight people I don’t like, it’s also people that are sick all the time (like, weak immune coughs and colds type of stuff).
Right now you’re on the internet instead of being physically active, that’s a health risk.
Who says I haven’t already gotten enough exercise today?
You’re aware of the concept of overworking your body, right?
Who says how much it’s acceptable to eat or drink?
I don’t care if you’ve gotten enough exercise, you would be healthier if you were walking around the block right now instead of sitting inside on the internet. Since my taxes pay for your medical bills I get to tell you how to live your life, so get walking!
come on guys, step over your ego.
Great, so maybe you can stop paying for my healthcare and I can stop paying for yours.
If were going to have a public health system, people should be required to take care of themselves
On the face of it, this sounds sensible. But, thinking more deeply, who should decide the required amount of care a person ought to take? Ideas about what it means to ‘take care of yourself’ are varied. And consider that some citizens of this country are simply unable to take the same personal health decisions that others have the privilege to take without a second thought.
What you’re talking about here isn’t a public system. A healthcare system that only serves certain chosen people is not public in any meaningful sense.
A public healthcare system is imperfect on the whole, but on average, when funded and administered properly, is structured to apportion care based on need, instead of the profit motive. I think that’s worthwhile, and the right thing for a society to do from a moral standpoint.
no one bothers that it is THE PEOPLE that pay for their health insurance, not the state.
the state made insurance mandatory, thats the only thing it is guilty of.
Thats a dark road to tread.
An example,
no alchol consumption is safe, so using your line of thinking you’d need to argue that anyone who partakes of alcohol at any anytime would fall under that line of thinking
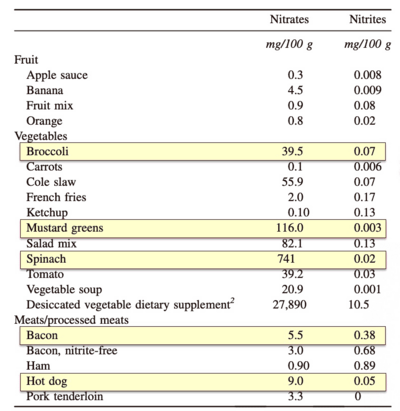
Processed red meats simailary, especially those treated with nitrites, so those eating bacon, ham etc shouldn’t be entitled to public heath care under your reasoning
Or are those things ok becase you do them ?
On the upside, now you’ve excluded 95% of the population, public healthcare will be cheap :)
Contra to most peoples thinking, if you’re concerned about public healthcare costs, you should “encourage” obesiety and smoking, they all die early, most health care coats are associated with healthy people in their old age. See here
https://www.nytimes.com/2008/02/05/health/05iht-obese.1.9748884.html
Adults are stupid and greedy, we all are.
it does not cost the state A DIME, because it is insurance that covers healthcare, not taxes.
The loss is unrealized potential of those who are sick. so, that means the state invested like 150.000 bucks in one citizen, in hopes to get like one million bucks out of them
(not out of them specifically, but out of their labour; it is a chain, you see, and the labourer pays taxes, the factory pays taxes when selling the product, the consumer pays taxes when buying the product, and so on)
alcohol and obesity by diabetis harm EVERY cell in your body, period. thats hard biochemstry, facts, it is the truth.
red meat, on the other hand, is quite unclear.
the studies involving red meat are interesting;
people self report by remembering long periods of time, a salami pizza counts as red meat, as does a whole mc donalds burger with fries on the side.
as for nitrate, this gets complicating. you seem to be on the right path. nitrates are a new topic for me, i never before read up on them:
https://www.diagnosisdiet.com/assets/images/5/nitrate-content-45165560.png
https://www.bbc.com/future/article/20190311-what-are-nitrates-in-food-side-effects
this is so tedious, no wonder everybody has a different oppinion
Perfect, let’s just get rid of public healthcare then
So I drink more pop than I should. Why should I have to pay more for my healthcare than my buddy who had a habit of timing running green lights as soon as they turned green. That isn’t illegal, either, yet it’s very risky behavior. It didn’t work out for him just one time, and he nearly died. Why should taxpayers have to pay for him?
The answer is because the vast majority of us engage in risky behavior, or just have the bad taste of passing on our poor genetics to the next generation, and the social cost for penalizing people for not agreeing with societal norms are too high. This includes drug use, even legal ones like alcohol. Sure, don’t spend limited resources such as donated livers on people who aren’t willing to make the lifestyle changes required to make it worthwhile, because someone else will probably have to die for that to happen. But if we could make new livers and the price was reasonable, I wouldn’t even be against that.
You should pay for their healthcare, because you have a contract with an insurance company.
What makes you think that I, posting in a Canadian community about a Canadian article, have a contract with a healthcare insurance company?
oh, sorry, there was much talk about public health insurance, i Of course don’t have a clue how that works in canada. sorry, my fault. I only focused on public health care, here in germany thats an insurance, i was ignorant.
Not a problem. It’s essentially rolled into our taxes for the most part in Canada. You may have health insurance on top of that, but that isn’t a guarantee and usually is a top-up of our universal coverage. This usually covers things like drug prescriptions, glasses, and hospital conveniences such as semi-private or private rooms. I agree with the general idea, though, that we as a group pay for everyone who is covered. My original point at the top of this thread is that removing people’s eligibility simply because of risky behavior can be very tricky and likely harmful to society.
If your buddy who likes gambling with green lights was convicted of a traffic offence as part of that accident he should have been on the hook for his own healthcare and the healthcare of anyone else he hurt.
Way to miss the point. It’s a good thing you don’t engage in any risky behavior, or anything that would have a negative impact on your health. I mean, it’s not like you would be a hypocrite, right?
I never said “Don’t engage in any risky behaviour”. Stuff like cardiovascular and lung diseases and Type 2 Diabetes doesn’t happen over the course of days, weeks, or months, you have to be chronically treating yourself like crap for years to get to those points.
Free climbers don’t usually die the first time, either.
Jesus Christ that’s fucked up. Only 36 too and stopped drinking… and had a willing living donor. What do you do in this situation when they won’t help you? Go down to Mexico?
Jesus Christ that’s fucked up. Only 36 too and stopped drinking…
From the article:
Amanda Huska died Aug. 15 after spending six months in an Oakville, Ont. hospital.
and:
Huska, he said, stopped drinking as soon as she was diagnosed with Alcohol Liver Disease on March 3
So that sounds like she was immediately admitted (which implies she was already very sick) and only was sober in the hospital. In my opinion, that doesn’t qualify for “stopped drinking” and unfortunately she didn’t get a chance to prove whether or not she was actually able to stop.
How much do you need to drink to get ALD at 36?
Typically, a huge amount. But genetics may have been an issue, as well.
I was reading through the article and I think the policy in question is this
Transplant guidelines in Ontario and much of Canada require patients with ALD to first qualify for a deceased donor liver. If they don’t meet that criteria, they aren’t considered for a living liver transplant, even if one is available.
Also this
“The sicker someone is, the more they benefit from getting an entire liver from a deceased donor, as opposed to part of the liver from a living donor,” said Dr. Saumya Jayakumar, a liver specialist in Edmonton and an Associate Professor in the Faculty of Medicine & Dentistry at the University of Alberta.
“On the off chance their (living) liver doesn’t work, they urgently get listed for a deceased donor,” said Jayakumar. "We need to make sure that everyone who is a candidate for a living donor is also a candidate for a donor graft as well, " she added.
As for why that is, I’m not familiar. I’ve asked someone else and I’ll edit in more if I learn more
There are more people who need transplants than there are organs, so the medical profession has to make decisions about who to deny. This was a reasonable decision, in my opinion.
I’d be inclined to agree, except that her partner wanted to donate HIS liver and was prohibited from doing so as a living donation due to the alcohol use determination.
In Canada, drinking more than 3 drinks per week is medically considered “high alcohol use” for a woman… (6 for a man). This limit keeps getting lower year after year
If this can prevent you from getting organ transplants, then it encourages lying to your medical doctor about your current habits… That lady was not considered alcoholic, she just used alcohol in greater amount than the limit considered acceptable by doctors.
Latest stats show that almost 4 out of 5 people has exceeds that limit at some point in their life. This woman died only because she was honest with her doctor about her alcohol use. (Note that the article says her partner was a compatible donor but the system refused to accept him because she used alcohol. It’s not about lacking donors.)
This woman died only because she was honest with her doctor about her alcohol use
No, and it even says so in the article
She quit about 5 months before her death when transplants require 6-12 months of sobriety. She was drinking regularly with the fucked up liver before that diagnosis, and liver damage isn’t something that just suddenly appears.
She kept drinking despite what would have been intense cramping pain and a slow death, thats why she was denied (addiction) and ultimately died
Note that the article says her partner was a compatible donor but the system refused to accept him because she used alcohol
And as the article also says it’s incredibly dangerous for someone to get a live-donor transplant when they’re in bad shape like she was, as failure of that means they’ll need to let her die on-table or transplant a good dead one into her (which she was denied for, due to her drinking)
It’s sad, but this woman died to alcohol abuse, pure and simple
That’s a lot of vague statements you’ve repeated from the article. What’s drinking “regularly” (this was before the diagnosis as you’ve stated)? “She kept drinking”, what does that mean? How much alcohol was she consuming? Did she have a sip of her friends wine and was honest about it so was rejected?
as the article also says it’s incredibly dangerous for someone to get a live-donor transplant when they’re in bad shape like she was, as failure of that means they’ll need to let her die on-table or transplant a good dead one into her
Where does it say that? You’ve completely twisted the statements.
“On the off chance their (living) liver doesn’t work, they urgently get listed for a deceased donor,” said Jayakumar. "We need to make sure that everyone who is a candidate for a living donor is also a candidate for a donor graft as well, " she added.
Huska’s time at the Oakville hospital likely cost over $450,000 - ($3,592 per day for ICU care) with an additional 61 days in a ward bed which likely cost about $1,200 a day, A liver transplant in Ontario is pegged at about $71,000 to $100,000 in Ontario based on data from 2019.
In 2021, 15.6 per cent of Canadians over 12 engaged in heavy drinking – a term defined as five or more drinks for males, or over four for females, on one occasion at least once per month in the past year.
Heavy drinking is drinking ONCE per month in the past year. If this is based off of before her diagnosis, you’re gonna exclude like 80% of the working population who actually does go out for drinks or private occasions (unless they just lie which I guess they should’ve in this situation). Between the price of keeping them alive but not fixing the problem and there being no “review” process for decisions, I would categorize this as a bad system that allowed a preventable death from an alcohol related disease to continue.
I’m quite torn on this issue, my sister donated her kidneys and liver when she died. On one hand people who need an organ, need an organ but on the other hand deceased persons organs are so rare that they should go to those with liver diseases they have no medical control over before those who are sick from an avoidable disorder.
I don’t like to think of my sister’s liver going to someone who would abuse it over someone who just happen to have a genetic liver issue. She lived a life too short bringing joy and education to many children, her final act saving others would be soured by someone wasting it.
Maybe if donating organs was compulsory they wouldn’t be so rare.
Yeah… no. Perhaps opt out by default, but not compulsory.
Why not? Why do you need the ability to deprive someone of a live saving procedure after you literally died?
I dont know. Probably because it risks being abused. The US already has private prisons filled to the brim with trivial felons forced to work in sweat shops… im sure theyll love to sell their organs too after dying from heat stroke.
I see, that’s a valid concern. I wonder whether we could try to prevent such abuse by automatically excluding more prone groups like prisoners. It really seems crazy to me how many organs, which could literally save someone’s life, are going to waste.
I think opt out would be sufficient. Right now, its a compilcated to opt in and not many people thinks about it. In my state, the only time you see it, is a small checkbox when you get a drivers license.
But being opt out everyone is included unless they choose not to, for whatever reason. Which is think is more than fair. Its their body, they should have the right to do whatever they wish, regardless if they arent using it anymore. The amount of people opting out would be a minority, so it shouldn’t really be a concern.
Do you mean opt in by default?
No, the current system is opt in. You have to choose to be a donor. Opt out means you have to choose not to be.
Hi, transplanted organ recipient here (heart in my case), please be an organ donor if possible, thanks.
Giving a donor liver to an alcoholic, who only quit drinking upon diagnosis? Hell no. There are people with 5+ years who still worry about relapsing. A year is a start. Being forced to quit? I’d have wished her good luck if they gave the liver, but the person who dies instead of her?
I’ve watched alcoholics die of liver failure. It is a horribly sad thing. But sobriety is a choice, and you don’t get to go back in time to make it. I’m not sure why this article is spinning this as cruelty from the transplant board instead of maybe, just maybe, highlighting the destructive role that alcohol plays in society. I wonder if a booze company pays their bills or something.
Removed by mod
That would be nice if we had an unlimited supply of livers to transplant. Give everyone a chance.
Unfortunately I’d still rather give whatever liver we have on hand to someone guaranteed not to wreck it immediately, because giving her a chance means taking away someone else’s.
Medical notes suggest she started drinking in her late teens and had tried – unsuccessfully – to quit. After periods of sobriety, she returned to alcohol, which could increase the risk of continued use after the transplant.
Allen says Huska registered for an addiction program early on in her hospital stay to stop drinking after she’s discharged. Hospital records also say she suffers from anxiety.
From the first article CTV made about this, linked in in the first sentence they posted. Seems like we need to actually fund mental health care in this country or something, because she’s obviously been struggling for a while. You can see how the board would weigh previous failed attempts to quit against her.
Removed by mod
Lol I quoted something from not just this article, but a second article they link to from the one above, but sure.
They blocked her, at least in part, because she was an active alcoholic who had not shown any signs of changing her behaviour outside of time inside the hospital. Something that would have weighed on their decision included medical information such as previous attempts to stop drinking. Mental health care, including healthcare for addictions, is lacking in Canada. You can’t force someone to go into rehab, but offering better care and options might have helped her in the past.
As said in the main article as well as the one I read, in order to qualify for a living donation you need to qualify for a full donation, because if something goes wrong you’ll need a full liver ASAP and get bumped to the top of the list.
Removed by mod
Are you trying to argue that alcoholism shouldn’t be a factor AT ALL for liver donations, or that living donations shouldn’t also need to meet the standard full liver donation standards?
Removed by mod
It’s incredibly sad to hear someone die of a preventable cause this young, but I can also somewhat relate with the people who reviewed her application.
If a living donor wouldn’t have been sufficient, they’ve now created two patients where they previously had one, and without improving the primary patient’s condition. It makes sense that a donor organ from a deceased donor would be preferable.
That said, the current requirement for the patient to meet deceased donor standards for transplantation to be eligible to use a willing living donor make no sense. Both situations should have their own unique criteria, given that a living donor situation involves different risks for both the patient and the donor than a deceased donor situation would incur.
Ultimately this whole situation boils down to a scarcity situation though. If we want to solve this, it will require more people to register themselves as a donor and a review of the eligibility criteria as soon as more donors are available.
And how prevalent and socially acceptable Alcoholism has become.
It’s not just acceptable, it’s encouraged by the province to keep people from rage quitting their lives here.
If you are going to make alcohol consumption a bar to a liver transplant without making alcohol illegal you should all go fuck yourselves. You had a drink and you should die should not be a thing.
How has Polievre not tried to capitalize on this tragedy to pitch his “your bank is a better death panel than the transplant math” plan yet? American healthcare is half his platform!
As a former American, you do not want the American Health Care System unless you are very wealthy. It is an expensive bureaucratic disaster. BC Health may be imperfect but at least I am not paying us$700/month for family insurance that might be accepted by the doctor/hospital that sees me in an emergency.
Using the most recent data from the Canadian Institute for Health Information on hospital bed costs (2016), Huska’s time at the Oakville hospital likely cost over $450,000 - ($3,592 per day for ICU care) with an additional 61 days in a ward bed which likely cost about $1,200 a day A liver transplant in Ontario is pegged at about $71,000 to $100,000 in Ontario based on data from 2019.
I’ve come to the realization the only ones getting us off the dark timeline is us. I’m in USA, ready and willing. Thinking through what beginning steps I can take.
I didn’t like the cost section, because it felt simplistic. The actual procedure might be “cheaper”, but it doesn’t take into account the long term costs if something goes wrong with the “cheaper” option. Living liver donation is different from say a kidney, you’re taking a part of someone else’s liver.
“The sicker someone is, the more they benefit from getting an entire liver from a deceased donor, as opposed to part of the liver from a living donor,” said Dr. Saumya Jayakumar, a liver specialist in Edmonton and an Associate Professor in the Faculty of Medicine & Dentistry at the University of Alberta.
“On the off chance their (living) liver doesn’t work, they urgently get listed for a deceased donor,” said Jayakumar. "We need to make sure that everyone who is a candidate for a living donor is also a candidate for a donor graft as well, " she added.
I worry people are going to see those numbers and run with them, even though there’s more to consider than that. Financial calculations in medicine are always difficult, and it feels dirty no matter what
The article is not clear. Is the $71k price listed the cost of the surgery itself or surgery + hospital stay?
If it is just surgery then it is a very unfair comparison since the ICU stay would have been needed in either case, and at least some of the days in the ward for recovery.
Plus living donation means the donatee needs recovery time and a bed as well.
So some rough numbers I found from places online for rough estimates. Also, the link the article has for bed costs is actually to a study on liver transplant costs.
On average, 25 days in hospital between pre/post transplant. Of that, seems like a few days (varies by person) is in ICU. So thats 50 days of beds for the two of them, with say a week of combined ICU time.
Plus two surgeries - the article only takes an average cost of liver transplants, which is not indicative of a second surgery needed for a living donor transplant.
That puts the cost up to ~240,000-300,000. That cost is close enough that I can see it not being a factor for the decision.
The provincial governments in charge of our single payor health care system made the conscious decision to keep the liquor marts open while banning in-person sales of tea kettles (and we call ourselves a commonwealth nation!) during a pandemic.
I think our single payor at least partially did this to themselves.
I’m pretty sure people would’ve stormed parliament if you banned alcohol sales.
@NightOwl brutal
I thought this was about kidneys instead of livers and was very confused.











{kind=link}